Take Away The Walls would like to celebrate OT month by introducing Megan Lambert OTR to the educational forum. I interview Megan where we discuss why children struggle sitting still, the change in outdoor playground equipment and how its changing child development, and things to look for if a child needs OT support.
Melanie Ingram: Hey Megan! Thank you so much for being here and sharing your Occupational Therapy experience with Take Away the Walls.
Megan Lambert: Hi! You are welcome, I am so glad to be here and talk about this with you.
Melanie Ingram: Usually when I have interviews, I start with having our guest share a little bit about their career and experiences to where they are now. When I first heard about Occupational Therapy (OT) was about 6-7 years ago I had a mentor mention a particular grasp that a student was doing, and she mentioned, “I’ll bring this up to their parent since the parent is an Occupational Therapist.” When I heard this I was really really confused because I thought, “What does being a therapist for peoples careers, and jobs have anything to do with a writing grasp?” but since then, I took time to learn what OT is all about and obviously you are not a therapist that talks to people about their jobs. SO would you mind elaborating a bit more on what OT actually is?
Megan Lambert: Of course, Occupational Therapy helps support people with their tasks, any task that they perform throughout the day. OT is very broad and there’s alot that goes into it but that’s what I love about it the endless possibilities.
Melanie Ingram: So you do lots of focusing on the whole body verses a particular section or one area?
Megan Lambert: OT has the mindset of , “What the goal is for that particular person?” but with children it is a little different. We get to work on the sensory processing and we get to touch on the mental, physical, spiritual, emotional regulation and focus on the whole body.
Melanie Ingram: I love that you are able to work with people on their whole self. Not very many industries really focus in on that. Can you tell me a bit more about your favorite part of OT?
Megan Lambert: I think my favorite part it is getting to form a relationship with the person and what they goals are for themselves. There was a little boy I worked with who was about 7 years old and he was getting made fun of because he couldn’t ride a scooter. After working with him he was able to successfully ride a scooter with his friends. Kids don’t understand why they can’t do something, all they know is they are struggling with this. That’s when OT comes in and we help with that skill they are wanting to work on and make it fun.
Melanie Ingram: Can you tell me a little bit about your current role as an OT?
Megan Lambert: Yes, so I collaborate with the families and the client and we focus on their goals. Either they have delays in development and we come up with strategies to either adapt or utilize rehab when considering their needs and goals.
Melanie Ingram: For our readers, can you elaborate more on ADAPT vs REHAB?
Megan Lambert: Adapt is when we use a method to adapt the activity or environment to enhance the client’s performance to complete the specific task. So for an example when using scissors we would use loop scissors. This supports clients that have weak grip or need to focus on hand control to be able to cut a piece of paper. Rehab is basically strengthening exercises that help support the child to help promote function. But we make it fun, so we do wheel barrel races and bear crawls. I had one child who couldn’t flatten their hand. Every day they came in we worked on flattening their hand to encourage flattening their hand, and the strengthening exercises such as wheel barrel races and bear crawls help support that. We start the day by gross motor movements and obstacle courses and then are able to go into the classroom and then we will sit down in a classroom. That’s one thing that I don’t really understand about education and having children sit in chairs. I couldn’t even do that! Are you familiar with heavy work?
Melanie Ingram: a little but please mention a little more for our readers
Megan Lambert: Heavy work is anything that has a push or a pull movement so picking up a heavy ball and moving it, pushing a wheel barrel. it helps with their sensory system and helps them focus. This helps them focus on fine motor.
Melanie Ingram: To add on that, I’m a huge advocate for allowing children to move to be successful but I have worked and observed in various classrooms. A couple years ago I worked at a program and an educator mentioned to me that they can’t have their students move around prior to sitting down for a lesson because they can’t calm down. So if the children can’t “calm down” what exactly is missing? It makes me wonder if the movement wasn’t long enough or the children required different movements to help them be successful.
Megan Lambert: That sounds more like a transitioning goal and that is something we work with everybody on.
Melanie Ingram: Is that like a goal that you see from parents, educators, administrators? Where do you typically see that goal being requested?
Megan Lambert: Actually everywhere, it is a common one. Most of the ones I was writing were for the children that had sensory processing goals. They would struggle transitioning from the gym to the therapy room and we would write specific goals for that transition. Many times we would use visual timers, sometimes provide a transitioning toy. It is a hard one for children to work through. It is even a hard one for adults. Imagine if we were running or moving and then being told to stop. How would that effect us as adults? We would kind of be scrambling around trying to focus on the next thing.
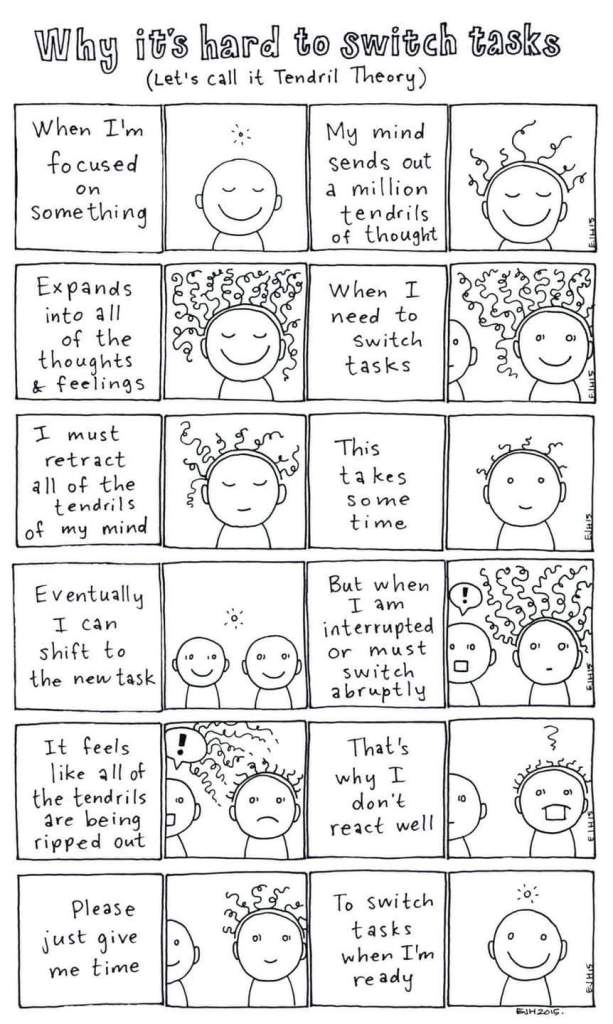
Melanie Ingram: There is this comic that I saw posted the other day and it’s called the Tendril Theory- it has a person working on a task and when being told to end something abruptly it essentially cuts off the “tendrils” and the person has a hard time reacting well.
Melanie Ingram: Over the past few years I’ve seen more children that require a need for OT. Especially in Kindergarten “The New First Grade”, children are sitting in desks more- but this is also due to Covid19 with social distancing and being 6 feet apart.
Megan Lambert: When you sent over the questions earlier I actually got really excited about this because I immediately thought of primitive reflexes.
Megan Lambert: We all have these reflexes ingrained in us since we were babies. There’s one called the Gallant Reflex. If you were to take your finger down a babies spine their pelvis will shift. This reflex helps them balance. After a few months the reflex slowly disappears as the baby grows and the movements are more controlled and voluntary. However, there are children who still have the primitive reflexes and their development is delayed. Another one is STNR that is another precursor to crawling; so anytime you flex your neck and your arms when getting up from the ground to crawl. If a person still has the STNR reflex after its supposed to already be integrated that child will struggle with concentrating, eye coordination, which also effects the handwriting.
Melanie Ingram: Basically the entire body is connected and if one part of the body isn’t integrated, delays will show up in various ways.
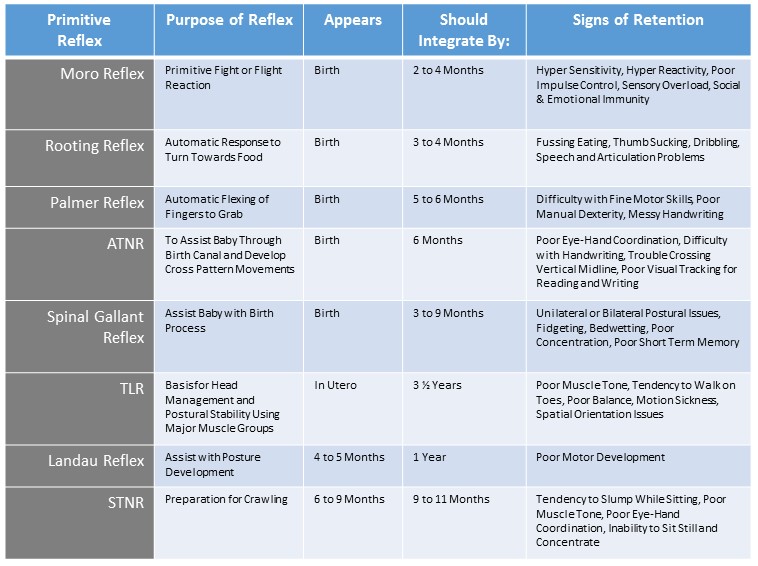
Megan Lambert: The good thing is, there are Occupational Therapy exercises that can be used to help develop the motor skill. Knowing the developmental milestones is very important for early intervention.
Melanie Ingram: From what we’ve discussed about OT there are lots of opportunities for gross motor play and movement. In the OT building there are things to hang on, swings, rock climbing etc. As we discussed there has been a shift in classrooms, where children don’t have the opportunity to move as much as they need to. I see materials being taken out of the classroom, out of the playground because its “dangerous”. This makes me concerned as an advocate for education because we are taking so many sensorimotor things out of the classroom because its considered dangerous and then asking ourselves, “Why is my child struggling with handwriting, and has poor coordination?” . Then we send them to OT to do the very things that were deemed dangerous in the classroom.
Megan Lambert: At the end of the day, children are going to do the movements that they need to receive the sensory input their bodies need, either at home or at school. That is really interesting though to hear the education side of things. Everything ties together, for the whole body development.
Melanie Ingram: That’s actually a topic I’d love to come back to in further detail with another article because there’s alot to unpack, but I’d love to hear a bit more about the senses.
Megan Lambert: There is a program called Astronaut Training Program, this was a sensory program I was trained on during a field experience. This helps with the vestibular system, and we would spin the children on these boards. There is this term called nystagmus, where your eyes move back and forth at a rapid pace and blurry vision, this happens especially after being spun around multiple times. Adults have a more developed nystagmus function and we get dizzy just looking at someone spin. Some children didn’t have that, others fell down and I had one that even threw up after being spun. We work through this vestibular exercise and it helps the child function better. Children spinning around on their own also helps support the vestibular system. I guess in a sense this circles back to our conversation earlier about taking away sensory materials- it would certainly be a disservice to the children.
Melanie Ingram: I honestly believe that every school and program needs to have an onsite OT, Applied Behavior Analyst, and a Speech Language Pathologist. I think it would be a huge help to programs and provide specific insight to human development that would help and benefit everyone. I had a child that needed heavy work, and after a little bit kinda gave up and then went back to their version of grounding seeking input.
Megan Lambert: It actually sounds like they needed a different form of heavy work and maybe if they did that activity a little longer they won’t *need* to be seeking that input anymore. If a child doesn’t want to do the activity, you have to come up with a way to work towards their goal in a different way. So for an example I had a child who loved anything batman and we ended up doing “batman races” to help them reach toward their goal. Usually if you find something that interests the child, they will be more excited to try the activity even if its hard. Also doing lots of encouragement and encouraging that hard work is okay too. Sometimes children don’t necessarily understand that hard work has to happen and everything doesn’t always come easy.
Melanie Ingram: If you could describe a typical day in OT in a *perfect* world
Megan Lambert: In a typical day in OT I look at the schedule of who my clients and I come up with a plan/goal for that particular child. Usually the goals are for a 6th month period. I use a software program called Clinic Source, it has a checkpoint and percentage of where and when the goal is being completed. I also input information such as progress notes, treatment and evaluation plan and plan of care. So if I had 8 kids to work with in the day I would be writing up 8 different plans. Usually goals aren’t completed immediately and they aren’t instant because children are still developing and this takes time.
Melanie Ingram: So you can’t just go into a room and say, “Child A has to work on developing their vestibular sense”. There is actually a whole process and plan.
Megan Lambert: Oh yes, when you show parents the scores it provides the evidence “this is why they need OT”. The results provide where they are developmentally based off of the average development.
Melanie Ingram: Are you allowed to give the evaluations or does a pediatrician provide them?
Megan Lambert: I do give the evaluations but the pediatrician does have to refer. There is certainly a profess to be referred to OT. They come in and I talk with the parents and I get information on the child, their needs and their interests. but also what the parents want as well.
Melanie Ingram: What would you say to look for if a parent or teacher thinks a child needs to be referred for OT?
Megan Lambert: I would start by encouraging them to familiarize themselves with the developmental milestones. You can find these on the CDC page. If a child is, lets say 6 years old and is performing gross motor skills as a 2 year old, I would recommend seeing the pediatrician to get referred to see an OT.
Melanie Ingram: Megan, I want to thank you for taking the time to speak on the forum. As you know, I truly believe that to help the whole child all professions that help a child should come together to support the child and their development. I know that I certainly learned alot through this time talking with you and I am sure others will learn as well.
Megan Lambert: You are welcome, thank you for having me!
Thank you so much for reading along, as and always, please be sure to rate, review and subscribe to help other educators and advocates alike to find support in this community.
Occupational Therapy Resource provided:
